Abstract
Background: 18F-FDG PET metabolic imaging provides significant help in the early diagnosis of inflammation of large and medium arteries, even before the appearance of structural vascular alterations. This retrospective study aims to evaluate the role of 18F-FDG PET in the diagnosis and management of large vessel vasculitis (LVV), including aortitis. Methodology: Fifty patients with clinical and/or biological suspicion of large vessel vasculitis but without a definitive diagnosis underwent 18F-FDG PET scanning. A qualitative visual scoring system and an average total vascular score (TVS) were used to compare 18F-FDG uptake in the vascular walls with that in the liver. Patients who had been on corticosteroids for more than 8 days were excluded from the study. Results: The study included 50 patients, 27 women and 23 men, with an average age of 65.8 ± 14.5 years. The analysis of 18F-FDG PET images allowed for the classification of subjects into two distinct groups. Among the 50 subjects, 16 (32%) showed higher 18F-FDG uptake in the vascular walls compared to hepatic uptake (PET-positive group), while 34 (68%) showed lower uptake (PET-negative group). In the positive group, 75% were diagnosed with Horton’s disease, and the remaining 25% with other inflammatory diseases such as Takayasu arteritis or polyarteritis nodosa. None of the subjects in the positive group had an aortic aneurysm. All patients with a positive 18F-FDG PET had elevated levels of C-reactive protein. The TVS obtained for aortitis alone was 5.9 ± 4.7, while the score for more global vasculitis was obviously higher, at 10.4 ± 6.3. Conclusion: 18F-FDG PET has become a valuable tool in the diagnosis of large vessel vasculitis, particularly in the early stages of the disease. It also allows for mapping of arterial involvement and estimation of disease severity using the TVS.
Keywords
18F-FDG PET, Aortitis, Large Vessel Vasculitis, Giant Cell Arteritis
1. Introduction
Large vessel vasculitis (LVV) involves the aorta alone and/or its main branches. It is characterized by inflammation of the walls of large arteries and manifests in two main variants: Takayasu arteritis (TA) and giant cell arteritis (GCA)
| [1] | Slart RHJA. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. 2018; 45(7): 1250-1269. https://doi.org/10.1007/s00259-018-3973-8 |
| [2] | Laurent C, Ricard L, Fain O, et al. PET/MRI in large-vessel vasculitis: clinical value for diagnosis and assessment of disease activity. Sci Rep. 2019; 9(1): 12388. https://doi.org/10.1038/s41598-019-48709-w |
| [3] | Antunovic L, Artesani A, Coniglio M, et al. [18F]FDG PET/CT in Large Vessel Vasculitis: The Impact of Expertise and Confounders on Image Analysis. Diagnostics. 2022; 12(11): 2717. https://doi.org/10.3390/diagnostics12112717 |
| [4] | Ben Shimol J, Amital H, Lidar M, Domachevsky L, Shoenfeld Y, Davidson T. The utility of PET/CT in large vessel vasculitis. Sci Rep. 2020; 10(1): 17709. https://doi.org/10.1038/s41598-020-73818-2 |
| [5] | van der Geest KSM, Treglia G, Glaudemans AWJM, et al. Diagnostic value of [18F] FDG-PET/CT for treatment monitoring in large vessel vasculitis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2021; 48(12): 3886-3902. https://doi.org/10.1007/s00259-021-05362-8 |
[1-5]
. Regarding various factors, such as age of onset, ethnic distribution, immunogenetic history, involvement of arterial territories, and characteristic therapeutic response of affected arteries, TA and GCA are different pathologies. Thus, giant cell arteritis predominantly affects Caucasians aged 50 years or older, unlike Takayasu disease which mainly affects populations under 50 years
| [6] | Samson M, B. Bonnotte B. How to apply the EULAR and ACR recommendations for the diagnosis and treatment of giant cell arteritis? Rev Med Interne 2022 Mar; 43(3): 135-138. https://doi.org/10.1016/j.revmed.2022.02.004 Epub 2022 Feb 21. |
[6]
. GCA is the most common inflammatory vasculitis in adults.
With an incidence of 20-30 cases per 100,000 individuals, which equates to 0.02% of the literature
| [7] | Balink H, Bennink RJ, van Eck-Smit BLF, Verberne HJ. The Role of 18F-FDG PET/CT in Large-Vessel Vasculitis: Appropriateness of Current Classification Criteria? BioMed Res Int. 2014; 2014: 687608. https://doi.org/10.1155/2014/687608 |
[7]
, the complications of LVV are potentially severe: increasing aortic dilation increases the risk of aortic dissection, while arterial occlusion increases the risk of ischemic damage to terminal organs such as the eyes, brain, or others.
Patients with LVV most often present with non-specific clinical symptoms, including back or chest discomfort, fatigue, weakness, weight loss, and fever. According to van der Geest et al.
| [5] | van der Geest KSM, Treglia G, Glaudemans AWJM, et al. Diagnostic value of [18F] FDG-PET/CT for treatment monitoring in large vessel vasculitis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2021; 48(12): 3886-3902. https://doi.org/10.1007/s00259-021-05362-8 |
[5]
, giant cell arteritis is also accompanied by cranial symptoms, particularly headaches and jaw claudication, while patients with Takayasu arteritis are more likely to present with limb claudication and loss of peripheral pulses
| [6] | Samson M, B. Bonnotte B. How to apply the EULAR and ACR recommendations for the diagnosis and treatment of giant cell arteritis? Rev Med Interne 2022 Mar; 43(3): 135-138. https://doi.org/10.1016/j.revmed.2022.02.004 Epub 2022 Feb 21. |
[6]
. In fact, there are two phenotypic presentations for giant cell arteritis, one cephalic and the other extra-cephalic. For example, rheumatoid arthritis (RA) is frequently associated with giant cell arteritis
| [6] | Samson M, B. Bonnotte B. How to apply the EULAR and ACR recommendations for the diagnosis and treatment of giant cell arteritis? Rev Med Interne 2022 Mar; 43(3): 135-138. https://doi.org/10.1016/j.revmed.2022.02.004 Epub 2022 Feb 21. |
[6]
. On the other hand, Takayasu disease can go unnoticed and be discovered incidentally at any age.
Regarding the histology of vascular lesions, GCA and TA also show considerable overlap of inflammatory tissue lesions
| [7] | Balink H, Bennink RJ, van Eck-Smit BLF, Verberne HJ. The Role of 18F-FDG PET/CT in Large-Vessel Vasculitis: Appropriateness of Current Classification Criteria? BioMed Res Int. 2014; 2014: 687608. https://doi.org/10.1155/2014/687608 |
[7]
.
High levels of inflammation markers such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are commonly observed at the time of diagnosis. However, if the biological inflammatory syndrome is almost constant in giant cell arteritis, it is inconsistent in Takayasu disease
| [6] | Samson M, B. Bonnotte B. How to apply the EULAR and ACR recommendations for the diagnosis and treatment of giant cell arteritis? Rev Med Interne 2022 Mar; 43(3): 135-138. https://doi.org/10.1016/j.revmed.2022.02.004 Epub 2022 Feb 21. |
[6]
.
A suspected diagnosis of LVV is based on clinical, biological, and paraclinical arguments. Particularly for GCA, the diagnosis is based on the presence, in a patient over 50 years old, of evocative clinical signs and a biological inflammatory syndrome, and the confirmation of the vasculitis diagnosis is provided by temporal artery biopsy. Nevertheless, GCA and TA show considerable overlap of inflammatory lesions of the vascular walls
| [8] | Slart RHJA, Nienhuis PH, Glaudemans AWJM, Brouwer E, Gheysens O, Geest KSM van der. Role of 18F-FDG PET/CT in Large Vessel Vasculitis and Polymyalgia Rheumatica. J Nucl Med. 2023; 64(4): 515-521. https://doi.org/10.2967/jnumed.122.265016 |
[8]
. The results of vascular imaging and the response to corticosteroid treatment also contribute to the diagnosis.
While antirheumatic drugs are increasingly used in the treatment of LVV, high-dose corticosteroids remain the reference treatment with the challenge of weaning. In TA, anti-TNF drugs are commonly used and in the maintenance treatment of GCA, anti-interleukin-6 receptor therapy has proven effective
| [5] | van der Geest KSM, Treglia G, Glaudemans AWJM, et al. Diagnostic value of [18F] FDG-PET/CT for treatment monitoring in large vessel vasculitis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2021; 48(12): 3886-3902. https://doi.org/10.1007/s00259-021-05362-8 |
[5]
.
18F-FDG PET metabolic imaging provides significant help in the early diagnosis of inflammation of large and medium arteries, even before the appearance of structural vascular alterations
| [4] | Ben Shimol J, Amital H, Lidar M, Domachevsky L, Shoenfeld Y, Davidson T. The utility of PET/CT in large vessel vasculitis. Sci Rep. 2020; 10(1): 17709. https://doi.org/10.1038/s41598-020-73818-2 |
| [5] | van der Geest KSM, Treglia G, Glaudemans AWJM, et al. Diagnostic value of [18F] FDG-PET/CT for treatment monitoring in large vessel vasculitis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2021; 48(12): 3886-3902. https://doi.org/10.1007/s00259-021-05362-8 |
[4, 5]
. The uptake of
18F-FDG on the walls of large arteries can be useful not only in diagnosis but also in disease monitoring and potentially in evaluating treatment response.
Several studies have shown good specificity of this imaging in diagnosing arterial involvement, with a sensitivity of about 89.5% for GCA and 87% for Takayasu arteritis (TA)
| [2] | Laurent C, Ricard L, Fain O, et al. PET/MRI in large-vessel vasculitis: clinical value for diagnosis and assessment of disease activity. Sci Rep. 2019; 9(1): 12388. https://doi.org/10.1038/s41598-019-48709-w |
| [9] | Soussan M, Nicolas P, Schramm C, et al. Management of large-vessel vasculitis with FDG-PET: a systematic literature review and meta-analysis. Medicine (Baltimore). 2015; 94(14): e622. https://doi.org/10.1097/MD.0000000000000622 |
| [10] | Gribbons KB, Ponte C, Carette S, et al. Patterns of Arterial Disease in Takayasu Arteritis and Giant Cell Arteritis. Arthritis Care Res. 2020; 72(11): 1615-1624. https://doi.org/10.1002/acr.24055 |
| [11] | Treglia G, Albano D, Dondi F, Bertagna F, Gheysens O. A role of FDG PET/CT for Response Assessment in Large Vessel Disease? Semin Nucl Med. 2023; 53(1): 78-85. https://doi.org/10.1053/j.semnuclmed.2022.08.002 |
[2, 9-11]
. Nielsen et al.
| [12] | Nielsen BD, Hansen IT, Kramer S, et al. Simple dichotomous assessment of cranial artery inflammation by conventional 18F-FDG PET/CT shows high accuracy for the diagnosis of giant cell arteritis: a case-control study. Eur J Nucl Med Mol Imaging. 2019 Jan; 46(1): 184-193. https://doi.org/10.1007/s00259-018-4106-0 Epub 2018 Jul 31. |
[12]
, have shown that sensitivity is lower in diagnosing craniofacial arteritis.
According to recent European and American recommendations
| [1] | Slart RHJA. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. 2018; 45(7): 1250-1269. https://doi.org/10.1007/s00259-018-3973-8 |
[1]
, for GCA with cephalic presentation or, with a cephalic-cervical ischemic complication, requiring urgent corticosteroid treatment, temporal artery biopsy should be performed first (gold standard, remaining positive for several weeks after the start of corticosteroid therapy, to avoid delaying treatment initiation). In case of a negative or non-feasible biopsy, a Doppler ultrasound of the temporal arteries, an angio-MRI, or an
18F-FDG PET could be proposed but only if corticosteroid treatment has not exceeded 5 days.
For GCA with extra-cephalic presentation, treatment initiation is less urgent due to fewer short-term complications. In these cases, given the invasive nature of temporal artery biopsy, imaging of the large vessels could be performed first.
For the diagnosis of Takayasu disease, imaging of the large vessels is proposed first. Imaging is also indicated in the search for isolated aortitis (present in 50% of GCA with cephalic presentation), with prognostic value due to increased risk of aortic aneurysm, relapse, or cardiovascular events (these can be exacerbated by corticosteroid therapy), associated with decreased survival compared to the general population
.
The objective of this retrospective study was to evaluate the contribution of 18F-FDG PET in the management of patients with inflammatory vasculitis, not only in diagnosis but also in classification and in the search for potential complications, and whether the same led to changes in therapeutic management.
2. Materials and Methods
This is a retrospective observational monocentric study. Diagnostic procedures were exclusively performed at the university hospital of Tours between March 2022 and August 2023. Patients on corticosteroids for more than 8 days were excluded. Clinical data, such as medical history, results of biological inflammation markers, and available results from temporal artery biopsy and echo-Doppler, were analysed.
Acquisition of PET Images
18F-FDG PET acquisition was carried out according to the internal standard procedures of the Nuclear Medicine Department of CHU Tours using a Vision 600TM tomograph (Siemens Healthineers). A fasting period of at least 6 hours was required before the IV administration of 18F-FDG. The dose of 18F-FDG was calculated based on the subject's BMI (BMI < 30, 2 MBq/kg; BMI > 30, 2.5 MBq/kg). Blood glucose levels were measured before the administration of 18F-FDG to ensure glucose levels were within an acceptable range (ideally not exceeding 1.26 g/l). All acquisitions were performed 90 minutes post-injection to increase the contrast between uptake in vascular walls and the blood pool. The acquisition protocol included a longer cranial image of 10 minutes.
Analysis of PET Images
The assessment of vascular uptake of 18F-FDG was visually classified by comparing it to that of the liver and mediastinum. Four grades were defined: 0 = no uptake (≤ mediastinum); 1 = low-intensity uptake (< liver but > mediastinum); 2 = intermediate-intensity uptake (similar to liver); 3 = high-intensity uptake (> liver); grades 2 and 3 indicate active VGV. Vascular uptake of 18F-FDG similar to or higher than that of hepatic parenchyma was interpreted as indicative of vascular wall inflammation.
Several arterial segments were examined. For aortitis, 5 segments of the aorta were analyzed: for the thoracic aorta, the ascending, descending, and arch segments, and for the abdominal aorta, the supra and infra-renal segments. For vasculitis, the arteries analyzed were the thoracic and abdominal aorta, carotid arteries, subclavian arteries, axillary arteries, iliac arteries, and femoral arteries. The uptake grade of each arterial segment was summed to obtain a Total Vascular Score (TVS), with values ranging from 0 to 21.
Statistical Analysis
The STATA software (Stata Corp., College Station, TX, USA, Version 17 for Windows) was used to analyze the obtained data. Descriptive analysis was conducted. Continuous variables were evaluated using the mean and standard deviation, while frequencies were used to analyze categorical data. We calculated the mean ± standard deviation and the necessary percentages to obtain the results. Continuous variables were compared using Student’s t-test, and for categorical variables, Pearson’s chi-square test was used. A p-value <0.05 was considered statistically significant.
3. Results
18F-FDG PET scans of 50 patients, 27 women, and 23 men, with a mean age of 65.8 ± 14.5 years (ranging from 35 to 89 years) were analyzed. Among the 50 subjects, 16 (32%) had
18F-FDG uptake in the vascular walls identical to or greater than that of hepatic parenchyma (positive PET group, +) and 34 (68%) had uptake lower than that of the liver (negative PET group, -). In the 16 PET+ patients, 10 were women, and the median age of this group was 72 years. In the PET- group, there were an equal number of women and men, 17, with a mean age of 63 years (
Table 1).
Table 1. Demographics, Clinical Symptomatology, and 18F-FDG PET Results.
| | 18F-FDG PET positive (n=16) N (%) | 18F-FDG PET Negative (n=34) N (%) | p |
Age (years) | Mean ± SD | 68.8 ± 12.1 | 64.6 ± 15.5 | 0.323 |
Range | 35-78 | 38-89 |
Median | 72 | 63 |
Sex | Female | 10 (62.5) | 17 (50) | 0.408 |
Male | 6 (37.5) | 17 (50) |
Corticosteroid | Yes | 5 (31.3) | 11 (32.4) | 0.938 |
No | 11 (68.7) | 23 (67.6) |
Start of corticosteroids (days) before PET | 0 | 11 (68.7) | 23 (67.6) | 0.287 |
3 | 1 (6.3) | 1 (2.9) |
4 | 0 | 1 (2.9) |
5 | 2 (12.5) | 4 (11.8) |
6 | 0 | 2 (5.9) |
7 | 2 (12.5) | 0 |
8 | 0 | 3 (8.8) |
Calcification (atherosclerosis) | Yes | 11 (68.7) | 15 (44.1) | 0.104 |
Not | 5 (31.3) | 19 (55.9) |
Biopsy | Negative | 8 (50) | 12 (35.3) | 0.028 |
Positive | 6 (37.5) | 5 (14.7) |
Not completed | 2 (12.5) | 17 (50) |
Treatment after PET scan | No treatment | 1 (6.3) | 20 (58.8) | 0.001 |
Continuation of corticosteroids | 5 (31.3) | 10 (29.4) |
Initiation of corticosteroid therapy | 9 (56.3) | 3 (8.82) |
Other | 1 (6.3) | 1 (2.94) |
Polymyalgia | Yes | 3 (18.8) | 8 (23.5) | 0.704 |
Not | 13 (81.2) | 26 (76.5) |
TIME | Yes | 12 (75) | 9 (26.5) | 0.001 |
Not | 4 (25) | 25 (73.5) |
Headache | Yes | 9 (56.3) | 13 (38.2) | 0.231 |
Not | 7 (43.7) | 21 (61.8) |
Hyperesthesia | Yes | 5 (31.2) | 4 (11.7) | 0.094 |
Not | 11 (68.8) | 30 (88.3) |
Jaw claudication | Yes | 4 (25) | 6 (17.6) | 0.544 |
Not | 12 (75) | 28 (82.4) |
Diplopia | Yes | 1 (6.2) | 6 (17.6) | 0.279 |
Not | 15 (93.8) | 28 (82.4) |
Fever | Yes | 4 (25) | 4 (11.8) | 0.234 |
Not | 12 (75) | 30 (88.2) |
Stroke | Yes | 1 (6.2) | 10 (29.4) | 0.065 |
Not | 15 (93.8) | 24 (70.6) |
Aortic aneurysm | Yes | 0 (0) | 2 (5.9) | 0.322 |
Not | 16 (100) | 32 (94.1) |
Cardiac stenosis | Yes | 2 (12.5) | 2 (5.9) | 0.421 |
Not | 14 (87.5) | 32 (94.1) |
CRP | Normal | 0 (0) | 19 (55.9) | <0.001 |
High | 16 (100) | 15 (44.1) |
Approximately 69% of positive patients had at least one vascular calcification plaque, while this rate was 44% in negative subjects. 14 PET+ patients underwent temporal artery biopsy, and histology confirmed vascular wall inflammation in 6. In the PET- group, 17 patients were biopsied, and the diagnosis of vasculitis was nevertheless confirmed in 5.
In the PET+ group, general condition deterioration, headaches, and hyperesthesia were the most frequent symptoms. None of the subjects in this group had an aortic aneurysm. All had elevated levels of C-reactive protein (CRP). In the PET- group, the main symptoms besides headaches and GCD were diplopia and a history of stroke, and only 56% had elevated CRP.
Table 2 presents the results of the analysis of positive
18F-FDG PET scans, notably the visual scores of
18F-FDG vascular uptake for the thoracic aorta and its main branches as well as TVS. The TVS for aortitis alone was 5.9 ± 4.7, and 10.4 ± 6.3 for more systemic involvement.
Table 2. Analysis of visual scores and TVS for the group of 16 patients with a positive 18F-FDG PET.
| | N (%) |
Visual Score | Grade 2 | 6 (37.5) |
Grade 3 | 10 (62.5) |
Vascular pathology | Horton's disease | 12 (75) |
Takayasu disease | 1 (6.25) |
IgA vasculitis | 1 (6.25) |
Vasculitis | 1 (6.25) |
Periarteritis nodosa | 1 (6.25) |
Diffuse vascular uptake of 18F-FDG | Yes | 12 (75) |
Not | 4 (25) |
Focal vascular uptake of 18F-FDG | Yes | 6 (37.5) |
Not | 10 (62.5) |
TVS for aortitis (mean ± standard deviation) | 5.88 ± 4.73 (Range= 0-15 Median = 5.5) |
TVS for vasculitis (mean ± standard deviation) | 10.44am ± 6.33am (Range= 2-21 Median = 11.5) |
Among the 16 PET+ patients, 12 had Horton’s disease, and 8 of these 12 patients had vascular uptake greater than that of the liver (67%).
The TVS for aortitis was 5.7 ± 4.8 and 6.5 ± 5.0, respectively, in patients with and without Horton’s disease. For vasculitis, the TVS was 9.5 ± 6.2 and 13.3 ± 6.9 respectively in patients with and without Horton’s disease (
Table 3).
Table 3. Metabolic characteristics of patients with (HD) and without Horton's disease (NHD).
| | HD (n=12) N (%) | NHD (n=4) N (%) | P value |
Visual Score | Grade 2 | 4 (33.3) | 2 (50) | 0.551 |
Grade 3 | 8 (66.7) | 2 (50) |
TVS for aortitis (mean ± standard deviation) | 5.7 ± 4.8 | 6.5 ± 5.0 | 0.778 |
TVS for vasculitis (mean ± standard deviation) | 9.5 ± 6.2 | 13.3 ± 6.9 | 0.322 |
For 5/16 PET+ patients, the scan was performed 4 to 8 days after corticosteroid administration. For these 5 patients, the number of affected vascular segments was lower compared to patients without corticosteroids.
31 of the 50 patients underwent temporal artery biopsy: 14 PET+ patients and half of the PET- patients. Histology confirmed the presence of vascular inflammation in 6 patients and was negative for 8 patients in the PET+ group. In the PET- group, histology showed no vascular wall inflammation in 12 patients but revealed inflammatory involvement in 5.
27 echo-Dopplers were also performed, 11/16 in the positive group and 16/34 in the negative group (
Table 4). In the PET- group, only two patients had pathological ultrasound, but for one the biopsy was negative, and for the other, it was not performed; for the remaining 14 with normal ultrasound, histology revealed a vasculitis pattern in only 2 cases. For the 11 PET+ patients who underwent ultrasound, among the 6 with negative ultrasound, 2 had histological confirmation of vasculitis. Among the 5 with positive ultrasound, only one had histological confirmation of vasculitis (biopsy was not performed in 2, and in 2 others it did not confirm the diagnosis).
Following the results of the 18F-FDG PET scan, corticosteroid therapy was continued in 5 patients in the PET+ group, 10 started it, and no specific treatment for the 16th patient.
Table 4. Results of biopsies and ultrasounds performed (US).
Positive 18F-FDG PET | Negative 18F-FDG PET |
US | Biopsy- | Biopsy + | Biopsy NR | US | Biopsy- | Biopsy + | Biopsy NR |
– (n=6) | 4 | 2 | 0 | – (n=14) | 14 | 2 | 4 |
+ (n=5) | 2 | 1 | 2 | + (n=2) | 2 | 0 | 1 |
NA (n= 5) | 2 | 3 | 0 | NR (n=18 | 18 | 3 | 12 |
NA: not achieved
4. Discussion
The main objective of this study was to evaluate the role of 18F-FDG PET in patients with suspected aortitis and/or large vessel vasculitis (LVV).
Large vessel vasculitis remains challenging to diagnose. In most cases, clinical symptoms and biological parameters do not allow for a definitive and precise diagnosis due to non-specific symptoms such as asthenia, anorexia, weight loss, fatigue, fever, night sweats, and elevated CRP levels. The combination of 18F-FDG PET metabolic imaging with structural imaging via hybrid PET/CT can provide significant assistance in diagnosing LVV by detecting arterial wall hypermetabolism.
Giant cell arteritis (GCA) and Takayasu arteritis (TA) are two types of vasculitis that primarily affect large arteries. Their clinical presentation, treatment, and prognosis differ. The treatment of these conditions has evolved with the increased use of other imaging modalities such as computed tomography (CT), ultrasound, and
18F-fluorodeoxyglucose PET, which have replaced angiography
.
18F-FDG PET is increasingly used as a screening tool, especially in complex clinical cases characterized by a fever and inflammatory syndrome of unknown origin. However, it is necessary to establish a robust, investigator-independent method for diagnosing LVV.
In our cohort, the studied population presented typical characteristics of inflammatory vasculitis, primarily GCA. This study shows that the most affected vascular segments were the brachiocephalic trunk (62%), aortic arch (60%), descending aorta (60%), and ascending aorta (72%), consistent with the results of several studies
| [10] | Gribbons KB, Ponte C, Carette S, et al. Patterns of Arterial Disease in Takayasu Arteritis and Giant Cell Arteritis. Arthritis Care Res. 2020; 72(11): 1615-1624. https://doi.org/10.1002/acr.24055 |
| [14] | Nassarmadji K, Vanjak A, Bourdin V, et al. 18-Fluorodeoxyglucose positron emission tomography/computed tomography for large vessel vasculitis in clinical practice. Front Med. 2023; 10: 1103752. https://doi.org/10.3389/fmed.2023.1103752 |
| [15] | Malich L, Gühne F, Hoffmann T, et al. Distribution patterns of arterial affection and the influence of glucocorticoids on 18F-fluorodeoxyglucose positron emission tomography/CT in patients with giant cell arteritis. RMD Open. 2022; 8(2): e002464. https://doi.org/10.1136/rmdopen-2022-002464 |
[10, 14, 15]
suggesting a higher likelihood of diffuse disease. No PET scan was performed if corticosteroid therapy was prolonged beyond 8 days. However, some patients had taken corticosteroids between 1 day and 8 days. For these patients,
18F-FDG PET did not show significant vascular metabolic activity, or the number of affected vascular segments was reduced even if the scan was considered indicative of vasculitis. In both groups, two-thirds of the patients were not on corticosteroid therapy.
Studies have reported that immunosuppressants could reduce
18F-FDG uptake within three days, or even one day, in the case of high-dose IV corticosteroid bolus, after the start of treatment, thereby reducing the diagnostic accuracy of
18F-FDG PET
| [16] | Taimen K, Salomäki SP, Hohenthal U, et al. The Clinical Impact of Using 18F-FDG-PET/CT in the Diagnosis of Suspected Vasculitis: The Effect of Dose and Timing of Glucocorticoid Treatment. Contrast Media Mol Imaging. 2019; 2019: 9157637. https://doi.org/10.1155/2019/9157637 |
[16]
. Some studies indicate that corticosteroid therapy does not alter the diagnostic accuracy of the scan, while others reveal that in patients suspected of LVV who had never taken corticosteroids, vascular 18F-FDG uptake was higher
| [7] | Balink H, Bennink RJ, van Eck-Smit BLF, Verberne HJ. The Role of 18F-FDG PET/CT in Large-Vessel Vasculitis: Appropriateness of Current Classification Criteria? BioMed Res Int. 2014; 2014: 687608. https://doi.org/10.1155/2014/687608 |
| [16] | Taimen K, Salomäki SP, Hohenthal U, et al. The Clinical Impact of Using 18F-FDG-PET/CT in the Diagnosis of Suspected Vasculitis: The Effect of Dose and Timing of Glucocorticoid Treatment. Contrast Media Mol Imaging. 2019; 2019: 9157637. https://doi.org/10.1155/2019/9157637 |
| [17] | Geiger KR, Pasvolsky O, Berger T, et al. Effect of steroid treatment on the diagnostic yield of baseline 18f-fluorodeoxyglucose positron emission tomography in aggressive B cell lymphoma. EJNMMI Res. 2022; 12: 59. https://doi.org/10.1186/s13550-022-00924-9 |
| [18] | Shelke AB, Aurangabadkar HU, Bradfield JS, Ali Z, Kumar KS, Narasimhan C. Serial FDG-PET scans help to identify steroid resistance in cardiac sarcoidosis. Int J Cardiol. 2017; 228: 717-722. https://doi.org/10.1016/j.ijcard.2016.11.142 |
| [19] | Influence of Steroid Treatment on 18F-FDG PET/CT Accuracy to Detect Vascular and Musculoeskeletal Involvement in Patients with Polymyalgia Reumatica. ACR Meeting Abstracts. Accessed December 15, 2023. |
[7, 16-19]
.
Unfortunately, histology was available for only 62% of the patients. In the positive PET group, 87.5% had a temporal artery biopsy, but this confirmed the diagnosis in only 12.5% of patients, or 6 out of 16, for whom 18F-FDG PET suggested an inflammatory pattern in the vascular walls. In the other group, biopsy results showed vascular inflammation in 5 patients and ruled it out in 12. These results can be explained by the fact that temporal artery biopsy remains positive longer under corticosteroid therapy than functional imaging (false negatives).
Diagnosing inflammatory vessels can be difficult if the temporal artery biopsy is negative or not feasible for ACG (extra-cranial phenotype) or TA, with diagnosis relying on a set of clinical-biological arguments and imaging, particularly metabolic imaging. Indeed, the reference treatment being glucocorticoids, known for their side effects, it is important to have a set of arguments to clarify the diagnosis before undertaking this treatment.
In cases of clinical suspicion of large vessel vasculitis in patients with vague, non-specific symptoms and elevated inflammatory markers, the use of
18F-FDG PET metabolic imaging should not be dismissed solely due to negative temporal artery biopsy results, ultrasound without arterial halo, or MRI without aortic wall thickening
| [7] | Balink H, Bennink RJ, van Eck-Smit BLF, Verberne HJ. The Role of 18F-FDG PET/CT in Large-Vessel Vasculitis: Appropriateness of Current Classification Criteria? BioMed Res Int. 2014; 2014: 687608. https://doi.org/10.1155/2014/687608 |
[7]
. In such conditions, PET allows for the search for differential or associated diagnoses (neoplasia, rheumatic disease, deep infectious focus), notably in our cohort, polymyalgia rheumatica (PMR) was often associated with positive PET (19%) but also with negative PET (23.5%), these results can explain the continuation of corticosteroid therapy despite the absence of vascular abnormalities on metabolic imaging.
Inflammatory markers also play an important role; in our cohort, a negative C-reactive protein level was associated with negative metabolic imaging.
Ultrasound also provides important information for the diagnosis of vasculitis. It is particularly useful in the assessment of superficial vessels but can also detect wall abnormalities of the aorta and its branches, combined with Doppler, which allows blood flow analysis. It is thus possible to visualize the temporal arteries in the context of Horton’s disease, which affects large and medium-sized arteries, typically in the cephalic region (temporal artery and its branches). In this study, a little more than 50% of the patients had an ultrasound examination. In both groups, most ultrasound examinations did not reveal vascular wall abnormalities. This proportion was higher for 18F-FDG negative patients (87.5%) than for the 18F-FDG positive group (55%).
In this study, the 18F-FDG positive group, consisting of 10 women and 6 men, had an average age of 72 years, mainly affected by Horton’s disease, while the negative group, consisting of 17 women and 17 men, had an average age of 63 years. Thus, these results suggest a predominance of the positive sex among patients with positive 18F-FDG PET.
A metabolic activity score, called the total vascular score or TVS, is based on the sum of visual assessments of 18F-FDG uptake in arterial segments. The total score ranges from 0 to 21, across various vascular regions, including thoracic, abdominal, subclavian, axillary, carotid, iliac, and femoral arteries.
In our study, the TVS for vasculitis was 13.3 ± 6.9 in patients without Horton’s disease and 9.5 ± 6.2 with Horton’s disease. It was lower, as expected, for patients with isolated aortitis: 5.7 ± 4.8 with Horton’s disease and 6.5 ± 5.0 without Horton’s disease.
18F-FDG PET is useful for early diagnosis of LVV, especially in the presence of non-specific symptoms
| [3] | Antunovic L, Artesani A, Coniglio M, et al. [18F]FDG PET/CT in Large Vessel Vasculitis: The Impact of Expertise and Confounders on Image Analysis. Diagnostics. 2022; 12(11): 2717. https://doi.org/10.3390/diagnostics12112717 |
| [20] | Blockmans D, de Ceuninck L, Vanderschueren S, Knockaert D, Mortelmans L, Bobbaers H. Repetitive 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: a prospective study of 35 patients. Arthritis Rheum. 2006; 55(1): 131-137. https://doi.org/10.1002/art.21699 |
| [21] | Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Takayasu arteritis and giant cell arteritis: a spectrum within the same disease? Medicine (Baltimore). 2009; 88(4): 221-226. https://doi.org/10.1097/MD.0b013e3181af70c1 |
| [22] | Bahrami M, Mohammadi H, Mirgaloyebayat H, et al. The role of 18F-fluorodeoxyglucose PET/computed tomography in the diagnosis and monitoring of large vessel vasculitides - a review article. Am J Nucl Med Mol Imaging. 2023; 13(4): 127-135. |
[3, 20-22]
. Molecular imaging has shown effective capacity to detect LVV for TA and GCA, according to a meta-analysis of 21 trials involving 413 participants. For GCA, the combined sensitivity and specificity were 90% and 98%, respectively. However, in individuals with TA, the pooled sensitivity and specificity were 84%, indicating lesser performance. Another meta-analysis yielded similar results, with sensitivity and specificity of 83.9% and 92.4%, respectively
| [23] | Lee YH, Choi SJ, Ji JD, Song GG. Diagnostic accuracy of 18F-FDG PET or PET/CT for large vessel vasculitis : A meta-analysis. Z Rheumatol. 2016; 75(9): 924-931. https://doi.org/10.1007/s00393-015-1674-2 |
[23]
. In our study, the total number of confirmed vasculitis cases based on 18F-FDG PET scan, biopsy and symptoms was 28. Among these, 16 patients (57%) had positive PET-CT results, while 12 patients (43%) had negative results. Our findings demonstrated a sensitivity of 57.14%, specificity of 100%, a positive predictive value (PPV) of 100%, and a negative predictive value (NPV) of 64.71%. When comparing our results to the existing literature, such as Nielsen et al.
| [12] | Nielsen BD, Hansen IT, Kramer S, et al. Simple dichotomous assessment of cranial artery inflammation by conventional 18F-FDG PET/CT shows high accuracy for the diagnosis of giant cell arteritis: a case-control study. Eur J Nucl Med Mol Imaging. 2019 Jan; 46(1): 184-193. https://doi.org/10.1007/s00259-018-4106-0 Epub 2018 Jul 31. |
[12]
, we observed a lower sensitivity. They reported a sensitivity of 64% and a specificity of 100%.
Following the results of the 18F-FDG PET scan, the clinicians decided to continue corticosteroid therapy for 5 patients in the PET+ group, and to start it for 10. For one patient, no specific treatment was initiated. Thus, 18F-FDG PET has conditioned therapeutic management.
For 11 of the 50 patients of our study, the PET scan request was based on recent stroke history related to possible vasculitis. For these patients, the clinicians immediately dismissed the need for biopsy. 18F-FDG PET results were negative for 10 patients and positive for 1.
This study nevertheless has limitations, including the lack of histological results for all included patients (temporal artery biopsy), selection bias (exclusion of patients on corticosteroid therapy for more than 8 days and those who accessed a particular acquisition protocol), 18F-FDG PET post-corticosteroid therapy was not performed, and the follow-up of these patients was not conducted.
5. Conclusions
This study highlights the diagnostic challenges of vasculitis, focusing on patients with 18F-FDG PET scans showing vascular inflammation. The integration of molecular imaging with clinical, biological, and histological evaluations provides a comprehensive approach to understanding vasculitis.
The 18F-FDG PET scan allows for the detection of inflammation in the walls of large vessels, particularly at the early stages of the disease. Our results highlight the likely effect of corticosteroids on the test results, with the risk of false negatives. To avoid this risk, we recommend performing PET scans before starting corticosteroid therapy or within three days of treatment.
These results highlight the need for further research with diverse populations to explore the optimal timing for 18F-FDG PET after corticosteroid therapy. Future studies should focus on standardizing imaging protocols and improving diagnostic accuracy, especially in complex cases. Research should also examine long-term outcomes to clarify the relationship between early diagnosis, treatment, and prognosis.
Abbreviations
LVV | Large Vessel Vasculitis |
TA | Takayasu Arteritis |
GCA | Giant Cell Arteritis |
CRP | C-reactive Protein |
ESR | Erythrocyte Sedimentation Rate |
BMI | Body Mass Index |
Author Contributions
Abrar Abdullah Bafail:Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft
Thibaut Carsuzaa: Writing – review & editing
Floriane Legot: Writing – review & editing
Maria-Joao Santiago-Ribeiro: Supervision, Writing – review & editing
Funding
This work is not supported by any external funding.
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix
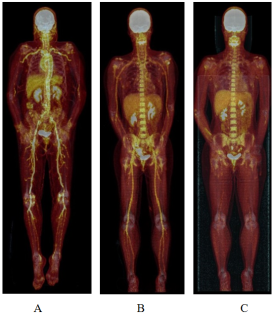
Figure 1. Here is an example of 18F-FDG PET in two patients with vasculitis: TVS of 15 for patient A and 8 for patient B. B1, examination before corticosteroid therapy, and B2 after 5 months of corticosteroid therapy and methotrexate.
References
| [1] |
Slart RHJA. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. 2018; 45(7): 1250-1269.
https://doi.org/10.1007/s00259-018-3973-8
|
| [2] |
Laurent C, Ricard L, Fain O, et al. PET/MRI in large-vessel vasculitis: clinical value for diagnosis and assessment of disease activity. Sci Rep. 2019; 9(1): 12388.
https://doi.org/10.1038/s41598-019-48709-w
|
| [3] |
Antunovic L, Artesani A, Coniglio M, et al. [18F]FDG PET/CT in Large Vessel Vasculitis: The Impact of Expertise and Confounders on Image Analysis. Diagnostics. 2022; 12(11): 2717.
https://doi.org/10.3390/diagnostics12112717
|
| [4] |
Ben Shimol J, Amital H, Lidar M, Domachevsky L, Shoenfeld Y, Davidson T. The utility of PET/CT in large vessel vasculitis. Sci Rep. 2020; 10(1): 17709.
https://doi.org/10.1038/s41598-020-73818-2
|
| [5] |
van der Geest KSM, Treglia G, Glaudemans AWJM, et al. Diagnostic value of [18F] FDG-PET/CT for treatment monitoring in large vessel vasculitis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2021; 48(12): 3886-3902.
https://doi.org/10.1007/s00259-021-05362-8
|
| [6] |
Samson M, B. Bonnotte B. How to apply the EULAR and ACR recommendations for the diagnosis and treatment of giant cell arteritis? Rev Med Interne 2022 Mar; 43(3): 135-138.
https://doi.org/10.1016/j.revmed.2022.02.004
Epub 2022 Feb 21.
|
| [7] |
Balink H, Bennink RJ, van Eck-Smit BLF, Verberne HJ. The Role of 18F-FDG PET/CT in Large-Vessel Vasculitis: Appropriateness of Current Classification Criteria? BioMed Res Int. 2014; 2014: 687608.
https://doi.org/10.1155/2014/687608
|
| [8] |
Slart RHJA, Nienhuis PH, Glaudemans AWJM, Brouwer E, Gheysens O, Geest KSM van der. Role of 18F-FDG PET/CT in Large Vessel Vasculitis and Polymyalgia Rheumatica. J Nucl Med. 2023; 64(4): 515-521.
https://doi.org/10.2967/jnumed.122.265016
|
| [9] |
Soussan M, Nicolas P, Schramm C, et al. Management of large-vessel vasculitis with FDG-PET: a systematic literature review and meta-analysis. Medicine (Baltimore). 2015; 94(14): e622.
https://doi.org/10.1097/MD.0000000000000622
|
| [10] |
Gribbons KB, Ponte C, Carette S, et al. Patterns of Arterial Disease in Takayasu Arteritis and Giant Cell Arteritis. Arthritis Care Res. 2020; 72(11): 1615-1624.
https://doi.org/10.1002/acr.24055
|
| [11] |
Treglia G, Albano D, Dondi F, Bertagna F, Gheysens O. A role of FDG PET/CT for Response Assessment in Large Vessel Disease? Semin Nucl Med. 2023; 53(1): 78-85.
https://doi.org/10.1053/j.semnuclmed.2022.08.002
|
| [12] |
Nielsen BD, Hansen IT, Kramer S, et al. Simple dichotomous assessment of cranial artery inflammation by conventional 18F-FDG PET/CT shows high accuracy for the diagnosis of giant cell arteritis: a case-control study. Eur J Nucl Med Mol Imaging. 2019 Jan; 46(1): 184-193.
https://doi.org/10.1007/s00259-018-4106-0
Epub 2018 Jul 31.
|
| [13] |
van der Geest K SM, Sandovici M, Bley TA, et al. Large vessel giant cell arteritis. Lancet Rheumatol.2024 Jun; 6(6): e397-e408.
https://doi.org/10.1016/S2665-9913(23)00300-4
Epub 2024 Apr 1.
|
| [14] |
Nassarmadji K, Vanjak A, Bourdin V, et al. 18-Fluorodeoxyglucose positron emission tomography/computed tomography for large vessel vasculitis in clinical practice. Front Med. 2023; 10: 1103752.
https://doi.org/10.3389/fmed.2023.1103752
|
| [15] |
Malich L, Gühne F, Hoffmann T, et al. Distribution patterns of arterial affection and the influence of glucocorticoids on 18F-fluorodeoxyglucose positron emission tomography/CT in patients with giant cell arteritis. RMD Open. 2022; 8(2): e002464.
https://doi.org/10.1136/rmdopen-2022-002464
|
| [16] |
Taimen K, Salomäki SP, Hohenthal U, et al. The Clinical Impact of Using 18F-FDG-PET/CT in the Diagnosis of Suspected Vasculitis: The Effect of Dose and Timing of Glucocorticoid Treatment. Contrast Media Mol Imaging. 2019; 2019: 9157637.
https://doi.org/10.1155/2019/9157637
|
| [17] |
Geiger KR, Pasvolsky O, Berger T, et al. Effect of steroid treatment on the diagnostic yield of baseline 18f-fluorodeoxyglucose positron emission tomography in aggressive B cell lymphoma. EJNMMI Res. 2022; 12: 59.
https://doi.org/10.1186/s13550-022-00924-9
|
| [18] |
Shelke AB, Aurangabadkar HU, Bradfield JS, Ali Z, Kumar KS, Narasimhan C. Serial FDG-PET scans help to identify steroid resistance in cardiac sarcoidosis. Int J Cardiol. 2017; 228: 717-722.
https://doi.org/10.1016/j.ijcard.2016.11.142
|
| [19] |
Influence of Steroid Treatment on 18F-FDG PET/CT Accuracy to Detect Vascular and Musculoeskeletal Involvement in Patients with Polymyalgia Reumatica. ACR Meeting Abstracts. Accessed December 15, 2023.
|
| [20] |
Blockmans D, de Ceuninck L, Vanderschueren S, Knockaert D, Mortelmans L, Bobbaers H. Repetitive 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: a prospective study of 35 patients. Arthritis Rheum. 2006; 55(1): 131-137.
https://doi.org/10.1002/art.21699
|
| [21] |
Maksimowicz-McKinnon K, Clark TM, Hoffman GS. Takayasu arteritis and giant cell arteritis: a spectrum within the same disease? Medicine (Baltimore). 2009; 88(4): 221-226.
https://doi.org/10.1097/MD.0b013e3181af70c1
|
| [22] |
Bahrami M, Mohammadi H, Mirgaloyebayat H, et al. The role of 18F-fluorodeoxyglucose PET/computed tomography in the diagnosis and monitoring of large vessel vasculitides - a review article. Am J Nucl Med Mol Imaging. 2023; 13(4): 127-135.
|
| [23] |
Lee YH, Choi SJ, Ji JD, Song GG. Diagnostic accuracy of 18F-FDG PET or PET/CT for large vessel vasculitis : A meta-analysis. Z Rheumatol. 2016; 75(9): 924-931.
https://doi.org/10.1007/s00393-015-1674-2
|
Cite This Article
-
ACS Style
Bafail, A.; Carsuzaa, T.; Legot, F.; Santiago-Ribeiro, M. The Role of 18F-FDG PET in the Diagnosis of Aortitis and Large Vessel Vasculitis. Int. J. Med. Imaging 2024, 12(3), 73-81. doi: 10.11648/j.ijmi.20241203.12
 Copy
|
Copy
|
 Download
Download
AMA Style
Bafail A, Carsuzaa T, Legot F, Santiago-Ribeiro M. The Role of 18F-FDG PET in the Diagnosis of Aortitis and Large Vessel Vasculitis. Int J Med Imaging. 2024;12(3):73-81. doi: 10.11648/j.ijmi.20241203.12
Copy
|
Download
-
@article{10.11648/j.ijmi.20241203.12,
author = {Abrar Bafail and Thibaut Carsuzaa and Floriane Legot and Maria-Joao Santiago-Ribeiro},
title = {The Role of 18F-FDG PET in the Diagnosis of Aortitis and Large Vessel Vasculitis
},
journal = {International Journal of Medical Imaging},
volume = {12},
number = {3},
pages = {73-81},
doi = {10.11648/j.ijmi.20241203.12},
url = {https://doi.org/10.11648/j.ijmi.20241203.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20241203.12},
abstract = {Background: 18F-FDG PET metabolic imaging provides significant help in the early diagnosis of inflammation of large and medium arteries, even before the appearance of structural vascular alterations. This retrospective study aims to evaluate the role of 18F-FDG PET in the diagnosis and management of large vessel vasculitis (LVV), including aortitis. Methodology: Fifty patients with clinical and/or biological suspicion of large vessel vasculitis but without a definitive diagnosis underwent 18F-FDG PET scanning. A qualitative visual scoring system and an average total vascular score (TVS) were used to compare 18F-FDG uptake in the vascular walls with that in the liver. Patients who had been on corticosteroids for more than 8 days were excluded from the study. Results: The study included 50 patients, 27 women and 23 men, with an average age of 65.8 ± 14.5 years. The analysis of 18F-FDG PET images allowed for the classification of subjects into two distinct groups. Among the 50 subjects, 16 (32%) showed higher 18F-FDG uptake in the vascular walls compared to hepatic uptake (PET-positive group), while 34 (68%) showed lower uptake (PET-negative group). In the positive group, 75% were diagnosed with Horton’s disease, and the remaining 25% with other inflammatory diseases such as Takayasu arteritis or polyarteritis nodosa. None of the subjects in the positive group had an aortic aneurysm. All patients with a positive 18F-FDG PET had elevated levels of C-reactive protein. The TVS obtained for aortitis alone was 5.9 ± 4.7, while the score for more global vasculitis was obviously higher, at 10.4 ± 6.3. Conclusion: 18F-FDG PET has become a valuable tool in the diagnosis of large vessel vasculitis, particularly in the early stages of the disease. It also allows for mapping of arterial involvement and estimation of disease severity using the TVS.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - The Role of 18F-FDG PET in the Diagnosis of Aortitis and Large Vessel Vasculitis
AU - Abrar Bafail
AU - Thibaut Carsuzaa
AU - Floriane Legot
AU - Maria-Joao Santiago-Ribeiro
Y1 - 2024/10/18
PY - 2024
N1 - https://doi.org/10.11648/j.ijmi.20241203.12
DO - 10.11648/j.ijmi.20241203.12
T2 - International Journal of Medical Imaging
JF - International Journal of Medical Imaging
JO - International Journal of Medical Imaging
SP - 73
EP - 81
PB - Science Publishing Group
SN - 2330-832X
UR - https://doi.org/10.11648/j.ijmi.20241203.12
AB - Background: 18F-FDG PET metabolic imaging provides significant help in the early diagnosis of inflammation of large and medium arteries, even before the appearance of structural vascular alterations. This retrospective study aims to evaluate the role of 18F-FDG PET in the diagnosis and management of large vessel vasculitis (LVV), including aortitis. Methodology: Fifty patients with clinical and/or biological suspicion of large vessel vasculitis but without a definitive diagnosis underwent 18F-FDG PET scanning. A qualitative visual scoring system and an average total vascular score (TVS) were used to compare 18F-FDG uptake in the vascular walls with that in the liver. Patients who had been on corticosteroids for more than 8 days were excluded from the study. Results: The study included 50 patients, 27 women and 23 men, with an average age of 65.8 ± 14.5 years. The analysis of 18F-FDG PET images allowed for the classification of subjects into two distinct groups. Among the 50 subjects, 16 (32%) showed higher 18F-FDG uptake in the vascular walls compared to hepatic uptake (PET-positive group), while 34 (68%) showed lower uptake (PET-negative group). In the positive group, 75% were diagnosed with Horton’s disease, and the remaining 25% with other inflammatory diseases such as Takayasu arteritis or polyarteritis nodosa. None of the subjects in the positive group had an aortic aneurysm. All patients with a positive 18F-FDG PET had elevated levels of C-reactive protein. The TVS obtained for aortitis alone was 5.9 ± 4.7, while the score for more global vasculitis was obviously higher, at 10.4 ± 6.3. Conclusion: 18F-FDG PET has become a valuable tool in the diagnosis of large vessel vasculitis, particularly in the early stages of the disease. It also allows for mapping of arterial involvement and estimation of disease severity using the TVS.
VL - 12
IS - 3
ER -
Copy
|
Download